NCCEH Spotlight: Low-cost body cooling strategies to tackle overheating during strenuous activity in hot environments


Practical and accessible cooling strategies for mitigating exertional hyperthermia in low-resource workplaces (O’Connor et al., 2026)
As periods of extreme heat become more common around the world, workers are increasingly at risk of heat-related injuries. In this systematic review, researchers from Australia and Canada evaluated practical and simple personal cooling strategies to address non-life-threatening hyperthermia (between 38°C and 40°C). While the review is focused on addressing overheating in workers, the results are applicable to other settings where strenuous activity increases the risk of overheating. This NCCEH Spotlight presents the highlights of the review.
Introduction
People’s core temperatures can rise due to two primary mechanisms. The first is passive exposure to heat from the surrounding environment, such as sitting in a hot room. The second is metabolic generation of heat, which happens when people exert themselves physically, through work or exercise. In addition, people can be exposed to passive heat while exerting themselves, a combination that can have a synergistic effect and further raise core temperatures (Figure 1).
Figure 1: Passive heat and metabolic heat influence on the body’s core temperature
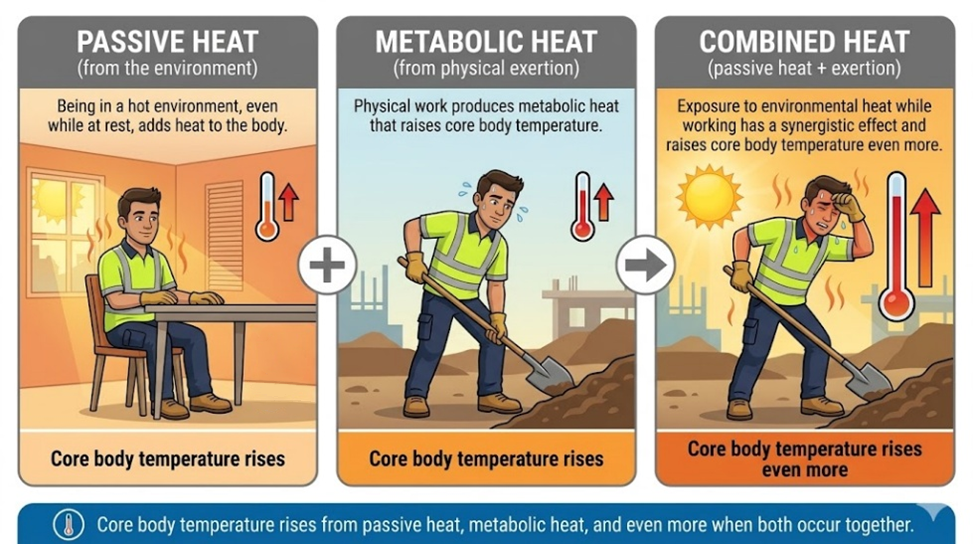
Hyperthermia is a condition where the body’s core temperature rises above a normal value of approximately 37°C. When core temperatures increase to 38-39°C, it can cause heat exhaustion and heat illness. Heat stroke is a severe and life-threatening form of hyperthermia that can occur when core temperatures exceed 40°C. Heat impacts people’s core body temperatures differently depending on factors such as age, gender, and health status.
On hot days, cooling strategies are needed to avoid heat-related illness and injury in workplaces and elsewhere. While air conditioning works well to prevent and reduce the impacts of hyperthermia, it is not universally available. Given the expected increase in the frequency of extreme heat events due to climate change, simple, accessible approaches to cooling are needed in workplaces and more broadly.
Research question and approach
The following question informed the systematic review by O’Connor et al.:
- What simple and practical personal cooling strategies can be used to treat people with non-life-threatening hyperthermia?
Several different types of studies were eligible for inclusion including randomized controlled trials, before-and-after studies, crossover, parallel and case series. Study participants were required to be healthy adults aged 18 or older and to be experiencing non-life-threatening hyperthermia due to physical exertion, in controlled laboratory environments or field settings.
Active cooling strategies were included if they were low-cost and could be implemented easily in the workplace. Ice water immersion was excluded as a strategy, given its impractical and costly constraints. Air conditioning was included as a comparator to assess how well the other interventions worked. A non-cooling comparator control was also included where study participants passively rested in the heat following hyperthermia without any active cooling intervention (passive cooling).
Key outcomes were rates of cooling in units of 1.0°C per minute (°C/min) and the time required (in minutes) to reduce body temperature by 1.0°C, measured by rectal probe or gastrointestinal telemetry. When the data allowed, meta-analysis was used to compare passive cooling strategy versus active cooling strategy. Meta-analysis is a method used to combine data from multiple studies to generate a single estimate of intervention effectiveness.
Primary findings
The review identified 145 studies, 129 of which were crossover design, 10 were parallel, five were pre-post design, and one was a case series. The studies all had small sample sizes, with a mean of 12 participants and standard deviation (SD) of 5 participants. The total number of participants across all studies was 1669, and 81% of participants were reported to be male. Most were young, healthy adults with a mean age of 26 years (SD=6). Almost all studies (n=121) were conducted in a laboratory, with the remainder (n=24) carried out in field settings. All studies used physical activity combined with heat from the environment to produce a state of hyperthermia. According to study inclusion criteria, heat from the environment may have been provided through laboratory conditions, or field settings like workplaces or sporting events. Excluding whole body immersion, cooling strategies were conducted in a range of wet bulb global temperatures, which is a standardized measure of combined air temperature, humidity, radiant heat, and air movement.
Twelve cooling strategies were analyzed across the 145 studies. Mean body temperature cooling rates (in °C/min), and the time needed to reduce body temperature by 1.0°C, are summarized in Figure 2.
Whole body immersion in cold (15 to <25°C) or tepid (≥25 to 28°C) water was the most effective strategy. All strategies except for limb immersion in tepid water (16 to 25°C) and the passive rest control had cooling rates similar to or better than air conditioning (0.03°C/min).
Figure 2: Weighted mean cooling rates and time to reduce core body temperature by 1.0°C of various cooling strategies
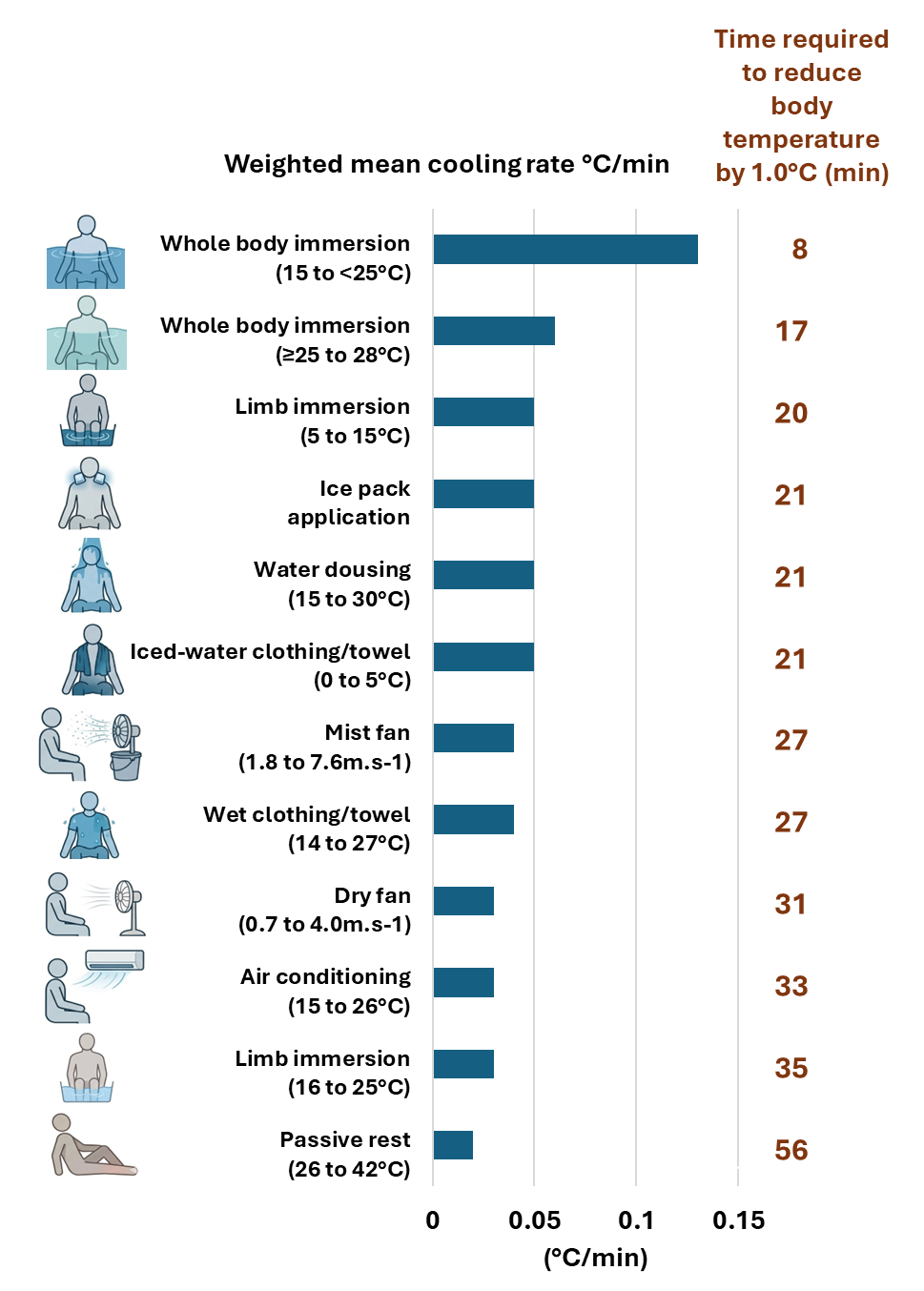
Note: Means are weighted by sample size. Cooling strategy temperature ranges are shown in brackets. For example, studies on water dousing strategies used water with temperatures ranging from 15 to 30°C.
Secondary findings
Meta-analyses
Forty studies included non-cooling controls, also known as passive cooling, such as sitting at rest in the same environmental conditions as the active cooling strategy. Only 26 of these studies were suitable to be included in meta-analyses. Cooling rates (in °C/min) for active cooling versus passive cooling strategies were compared for limb immersion, ice application, ice towels, dousing with water, mist fanning, dry fanning, and whole-body immersion. Limb immersion was the only method that showed significantly faster cooling (p=0.041) compared with passive rest. The rate of cooling for limb immersion was 0.05°C/min (95% confidence interval [CI]: 0.02, 0.06) compared with 0.02°C/min (95% CI: 0.00, 0.03) for passive rest. However, there were very few studies included in many of the meta-analyses, which makes it challenging to detect statistically significant differences due to the limited power of the analyses. For example, whole-body immersion showed faster cooling than passive rest, but the p-value for the analyses was greater than the critical 0.05 threshold.
Evidence gaps and limitations
The authors of this systematic review highlighted the following limitations of the findings:
- There are many individual and environmental factors that will modulate effectiveness of any cooling strategy, and caution should be taken in interpreting the generalizability of these results.
- The research participants were mostly young, healthy, male adults; there is a need to have more research on females, those with underlying chronic health conditions, and older adults.
- More controlled studies designed to compare strategies are needed, and more studies should focus on combined cooling strategies.
Implications for environmental health practice
Evidence from this systematic review highlights several simple, practical, and portable cooling strategies that may help to address exercise-induced and non-life-threatening hyperthermia. While these methods are not sufficient to treat clinical heat stroke, they do offer options to interrupt the progression of hyperthermia. Most of these strategies have favourable effects within 30 minutes, and many do not require electrical supply, which makes them applicable in a variety of settings.
The most effective strategy was whole body immersion in cold or tepid water; however, there are some practical limitations and safety considerations with this strategy. Beyond the need for further research on at-risk populations mentioned above, additional study is also needed for children and adults participating in activities such as school sports days or race events, where physical exertion may increase susceptibility to heat‑related illness and injury.
Additional resources:
- Extreme heat check tool video (Video, NCCEH, 2025)
- Weather impact guides (Environment and Natural Resources Canada, 2025)
- Indoor overheating: A review of vulnerabilities, causes, and strategies to prevent adverse human health outcomes during extreme heat events (Article, NCCEH, 2024)
- Extreme heat health check tool (Guide, NCCEH, 2023)
- Preventing indoor overheating (Subject Guide, NCCEH, 2023)
- Extreme heat (Subject Guide, NCCEH, 2022)
- Preventing injuries and deaths during extreme heat events (Webinar, NCCEH, 2022)
AI statement
AI tools were not used in the writing of this document, but AI image generation tools were used in the creation of Figure 1 and Figure 2.







